Rethinking SAT & ACT Preparation
UnpublishedLinda Narun, SLP
 Parents of students with special learning needs (LD or ADHD) are usually proactive in obtaining special programs and educational settings to meet the needs of their children. Tutors, special classrooms, or modifications are obtained. For some reason when enrolling students in SAT/ACT preparation classes we often forget that these same students do not learn well in conventional settings. The manner in which information is presented or the speed at which it is presented result in many students becoming overwhelmed and passive. Their anxiety increases and ultimately little is gained.
Parents of students with special learning needs (LD or ADHD) are usually proactive in obtaining special programs and educational settings to meet the needs of their children. Tutors, special classrooms, or modifications are obtained. For some reason when enrolling students in SAT/ACT preparation classes we often forget that these same students do not learn well in conventional settings. The manner in which information is presented or the speed at which it is presented result in many students becoming overwhelmed and passive. Their anxiety increases and ultimately little is gained.
We think that SAT preparation courses should, as in all other therapy we do, embrace the whole student rather than simply acquiring vocabulary and some test taking strategies. While these issues are very important, not all courses consider how to facilitate this learning. Many students, in addition to their learning needs, suffer from anxiety or ADHD which interferes with the ability to implement what they learn.
We are aware that students who have experienced some failure may have developed test anxiety. Each student’s learning style is a little different; so different learning strategies should are devised for each student.
The rate of teaching should be modified so that the student does not feel overwhelmed, and therefore, become passive. An increasing sense of involvement and success leads to active participation in the learning process.
The use of computers and technology is now used to help the students learn and evaluate the progress being made. Practice test results are analyzed by the instructor and student together so that errors become learning opportunities. With a sense of control over the learning, motivation increases. As training proceeds, the instructor should be sensitive to skill deficits that go beyond the SAT itself. These cognitive and academic skill deficits should be addressed separately.
We have been testing and teaching students with special needs for many years. The understanding of the specific learning needs together with their understanding of how students learn allow us to provide specialty training for students. Contact Linda Narun at This email address is being protected from spambots. You need JavaScript enabled to view it. or Lynn Ayres at This email address is being protected from spambots. You need JavaScript enabled to view it. for more information about this and all our programs.
The Fourth of July is just around the corner, but for many of you Independence Day will truly come some time in late August when you leave home for your first year in college. Just think: no more parents telling you to go to bed, telling you to wake up, making sure you finish your homework, and getting you to your appointments on time.
That’s a good thing… right? For many outgoing college freshmen, this level of independence and self-management may be difficult to navigate on top of all the other pressures that come with college. Hopefully you’ve been working to take over some of these responsibilities before that fateful date where you fly from (or get kicked out of) the nest. But even if you’ve got some of the basics down, independence can be a little overwhelming.
Over the years I’ve adopted a few tricks that I use to keep me on track and keep my ADHD from derailing me. It took a lot of trial and error to figure out how my brain works and how I can be prepared for any situation. I’ll be the first to admit that it’s an ongoing process, and I feel like my clients teach me as much as I teach them. So I thought I’d put together a Survival Guide – made up of some of the tools I’ve picked up along the way, and some of the tools that you, my clients, have recommended to me.got some of the basics down, independence can be a little overwhelming.
1. Smart Watch
The wristwatch was recently listed in an article on obsolete gadgets. Sure enough, I started looking at my teen clients’ wrists and I rarely see anything other than rubber bracelets. When I ask how they keep track of time, I hear one of two things:
1. “My phone.”
2. “I don’t.”
A good watch can give you a wake-up call, remind you of appointments, and remind you to take your medication. Oh yeah - it can also tell time and keep you on schedule. Tom Coughlin, head coach of the New York Giants famously quipped, “If you’re on time, you’re five minutes late.” Don’t be that guy. These new Smart Watches sync with your phone to keep you alerted to incoming calls, texts, and remind you of your schedule.
Suggestions: Coo Koo Watch ($129: Apple), Sony Smart Watch ($129: Android)
 ß
ß2. Smart Phone
I know, I know. Thanks, Captain Obvious. Telling my clients to carry a smart phone is like telling them to breathe. But I include it on this list for what it can do beyond texting, Instagram, and iTunes – namely, keep you organized. There are hundreds of organizer apps out on the market (Apple and Android) that can help you keep tabs on your tasks. You can set a reminder for an appointment, call to confirm, and bring up a map of the location all within a couple of clicks.
I recommend: Things ($50: Apple) , AnyDo (Free: Apple, Android)

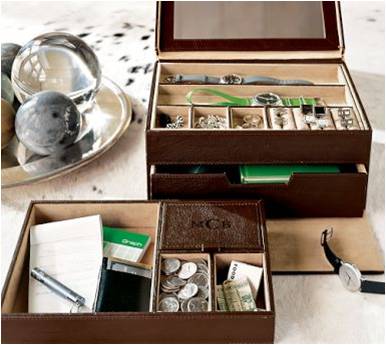
3. Valet
The average American spends 55 minutes a day looking for misplaced items. That’s 14 days per year that you can never get back just because you can’t remember where you put your keys. A valet isn’t just a guy who parks your car. It’s also a stylish organizer for your dresser or your bathroom counter where you can throw your keys, wallet/purse, and phone at the end of the day.
I recommend: Amazon.
4. Corkboard/Dry Erase Board
You need a place to keep track of bills, appointment reminders, and your roving to-do list. The corkboard lets you get things up and off of your desk, but in a place that’s right around eye level. Use the dry erase board to write down phone numbers, quick notes, and reminders until you can transfer them to your organizer (see #2).
Suggestions: These can be found at any office supply store, such as Office Depot, Staples, etc.\\
5. Man-Bag (aka “Messenger Bag” or “Murse”)
You need a way to carry around all of your stuff and it’s time to take a page out of the ladies’ handbook, gentlemen. Until cargo pants come back into style, your best bet is a Man-Bag. It has plenty of room for your tablet/laptop, paperwork, iPod, and that book you never have time to finish. The Man-Bag used to get a bad rap for being feminine, or “sissy.” Not anymore. Unless, of course, you think that marrying a super-model and winning a bunch of Super Bowls is sissy.
{kind=link}
I recommend: Target ($20 range), Banana Republic ($100 range)

With all of this tech that I’m pushing on you, this item is the cheapest and possibly most essential item in your Survival Kit. I learned this one from my dad, who always keeps an index card and a pencil in his shirt pocket to write down things that come to his mind. Whether you jot down a reminder to run to the bank, a quick grocery list, or someone’s phone number, the old pad and pen is a throwback that has aged beautifully. But Dr. Peacock, you say, why would I use a pad and pen when I just downloaded that organizer app for my phone? Because, I respond, what if you’re on your phone when you are given the information that you need to write down? That’s why. Trust me on this one.
Suggestions: Pick one up when you’re getting your cork board
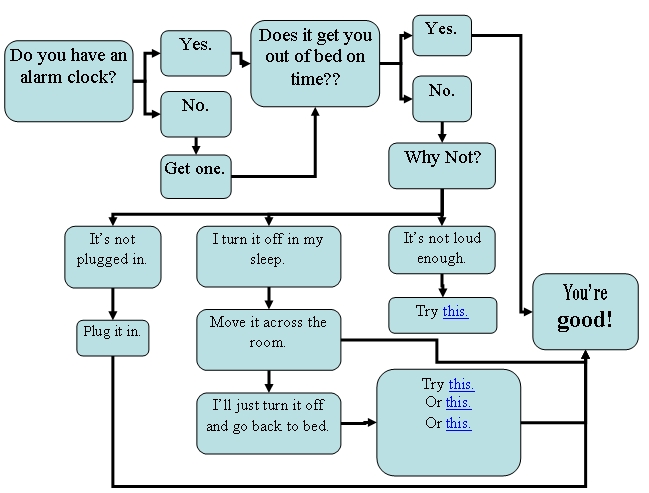
7. A Wake-Up Call
Even though it’s the last item on my list, this is really the first step in Self-Management. If you can’t get yourself out of bed in the morning, the rest of this is moot. And if you can’t get yourself out of bed, you’re not alone. One of the biggest reasons that students struggle in their freshman year is that they don’t make it to class. Follow this handy-dandy flowchart to help you figure out which alarm clock is right for you.

W. Walker Peacock, Psy.D. and Julie Sherman, Ph.D.

Applied behavior analysis is commonly used as a way to reinforce appropriate behaviors and discourage inappropriate behaviors through consequences. That is all fine and good, but what happens when your child doesn’t do that desired behavior AT ALL? If a behavior never occurs, it is not in the person’s repertoire. Shaping is the process of adding behaviors to a person’s repertoire. Shaping is used when the target behavior does not yet exist.
The key to shaping is reinforcing your child as he or she gets closer and closer to the end goal. In playing, “Hot & Cold,” you reinforce any movement that takes the player closer to the prize. Each movement is a closer approximation of the desired behavior. If the prize is under the couch, and the player is moving towards the couch, you yell, “hotter,” and reinforce the behavior. If the player moves away from the couch, you yell, “colder” (not reinforcing).
Shaping is a process that we have learned all throughout our lives. When we were babies, we went from rolling over to scooting, crawling, standing up, taking those first steps, walking, and running with ease. We were reinforced for these big steps in our lives through praise from our parents and caregivers. They were so excited that we were able to move forward and reach those milestones. We were successful. The same is true for so many other things: toilet training, eating independently, learning how to dress ourselves, social skills, time management, communication for both verbal and nonverbal individuals, and learning how to use our iPads, iPhones, and computers. These are skills that most of us take for granted. In reality, though, each is quite an accomplishment when you consider the number of skills it takes and how many steps are involved that you need to learn beforehand.
Let me give you an example. Jacob’s mother really wants him to learn the responsibility of cleaning his room. There has always been a maid in the house, and Jacob has never learned how to organize his things. In this case, it would be unfair to expect Jacob to clean his room spotless, or as well as the maid. Instead, the first step might be to reward Jacob for going into his room when his mother told him to. The next step might be to reward him for putting several things in their place as his mom directs him where things go. Then, reward him for putting things on the shelf by himself, even if it is put on the shelf in a careless way. Gradually increase the expectations for cleaning until Jacob’s cleaning his room looks similar to how the maid cleaned.
In another example, Ben throws a tantrum at school whenever he is frustrated with his work or does not know how to solve a problem. His tantrums are violent and may involve throwing tables and/or screaming. Shaping for this behavior would involve creating a new, more appropriate response for solving problems and dealing with frustration- asking for help. Ben’s teacher might start by rewarding Ben when he makes a sound, “Ben, I hear you making a noise. Would you like some help?” Once Ben is making this noise consistently, his teacher would modify the reward criteria, “Ben, say, ‘Help.’ Great job saying, ‘Help.’ What do you need help with?” Gradually increase the amount of words required for a reward, and eventually, Ben will be using a complete sentence to ask for help. Finally, reward him for raising his hand before asking. Each step gets you closer and closer to the end goal, replacing his tantrums by creating a more appropriate way to get what he needs.
Shaping can be used for any behavior that you do not see now, but that you would like to see in the future. It can also be used to make behaviors more precise. Among other things, shaping works well for improving symptoms associated with ADHD such as increasing attention span or decreasing hyperactivity. Let’s say that Sarah is able to attend to a task for approximately 10 minutes before she is distracted. Initially, shaping would require Sarah’s parents to reward her for paying attention for 10 minutes. The next week, the criteria for reward might increase to 11 minutes, and the next week to 12 minutes. The criteria would increase over time until Sarah’s attention span has improved to a manageable level. For hyperactivity, you might try to increase the amount of time that Sarah stays seated.
Sleeping alone in the dark is also a good example. Jenny is scared of the dark, and her mother often lies down with her at night until she falls asleep. There are two ways to handle this, both involving shaping. The first way is to remove mom from the room and reward Jenny for lying in bed by herself, with the light on. Jenny’s mother would, over time, make the room darker and darker until Jenny is sleeping in the dark by herself. This would be ideal if Jenny’s room had a dimmer. The second way is for Jenny’s mother to move closer and closer towards the door and away from the bed. The first week, Jenny’s mom might sit on the bed instead of lying down, and the next week, she might sit on the floor by the bed. Eventually, Jenny will be alone in the room sleeping by herself in the dark.
Many young adults have difficulty launching, going out into the world, and successfully moving on to college or a career. Shaping may be appropriate for this situation if the barrier to moving forward is anxiety. For example, John’s parents give him an allowance each month for him to pay rent, buy groceries, etc., and John has a hard time leaving his house because of his anxiety in social situations. He currently leaves his house three times each week. When using shaping, this young adult might be given homework assignments that gradually build toward helping him to become more independent. First, John would be rewarded for going out three times a week, then four times a week, until he is leaving his house everyday of the week. Next he might be rewarded for going to volunteer at an animal shelter or food bank. The expectations would slowly increase until John is able to work independently at his own job and provide for himself.
Rules for shaping:
- Define the target behavior: The behavior you want hasn’t occurred yet. It is the end goal, so you must decide what behavior is to be “shaped.” To get to the target behavior, you must have a clear idea of what it is.
- Reinforce successive approximations of the target behavior: Shape your child by rewarding him for getting closer and closer to the desired behavior. Reinforce an approximation several times or until a closer approximation appears, whichever comes first. If he gets stuck at a particular step, induce variability by withholding reinforcement. He will try new things to get the reward, and some of the new behavior will be in the direction that you want the behavior to go. Reward it! In general, shaping progresses more rapidly when increases in the requirements for reinforcement are small. Don’t hold out for big advances.
- Monitor results: The only way that you can tell if you are successful at shaping behavior is by noting any changes in behavior. Are you seeing progress towards the desired behavior? Is the behavior that occurs now closer to the target behavior than when you started? Is it time to hold out for a closer approximation?
Please feel free to contact me or the Tarnow Center if you have any questions about creating new behaviors in your child, adolescent, or young adult. We have Child Psychiatrists and Child Psychologists in Houston and Sugar Land.

Twenty years ago I had an enjoyable dinner with Patrick Carnes, PhD. He is the foremost authority on Sexual Addiction. Patrick J. Carnes is a nationally-known speaker on addiction and recovery issues. He is the author of Out of the Shadows, Contrary to Love, A Gentle Path Through the 12 Steps, and Don't Call It Love. He is the clinical director for sexual disorder services at The Meadows in Wickenburg, Arizona. Carnes is the editor-in-chief of Sexual Addiction and Compulsivity: The Journal of Treatment and Prevention, the official journal of the National Council of Sexual Addiction/Compulsivity, an organization for which he also serves as a board member. He also serves on the national advisory board of the American Academy of Health Care Providers in the Addictive Disorders.
He started a program at the Meadows Treatment Center noting that this was indeed an addiction that was being overlooked and undertreated. As most of you probably know he was right. He wanted to meet with me because he was trying to understand the biologic components of this addiction. He heard about my work with ADHD patients over the life cycle and wanted to understand how ADHD could be a contributing factor. We both agreed that that indeed we were both seeing this phenomenon. Patients with ADHD had more addictions in general and that sexual addiction was a real problem. We also discussed that the Internet would create a major stimulus for Pornography Addiction. We predicted that the Internet now brought pornography into the home and that adolescents would now be able to access any perversion or sexual act they could think of and many they never dreamed of. Suddenly this media blossomed. Today the number 1 Internet search is for pornography. It is the biggest business on the Internet. So now we have Pornography Addiction as well as Video game addiction.
Patients with ADHD have a higher incidence of drug addiction also. Cigarette smoking is twice the risk with ADHD and individuals start a younger age as well as have greater difficulty stopping. This association is found with all substance abuse disorders. Dr. Kafka, Clinical Associate Professor at Harvard, research shows that Hypersexual Disorder and ADHD have a 17-19% association. Dysthymia was the most common co-existing axis I disorder n Hypersexual Disorder patients, occurring 61-62% of the time, followed by alcohol abuse(25-39%) and Social Phobia(22-25%). Bipolar Spectrum Disorder is also highly associated (26%) with Hypersexual Disorder.
The reason that ADHD and Sexual Addiction are associated is multifactorial. ADHD is always seeking something novel when they are bored or depressed. They also use sex as a way to relieve stress, which they often create in their lives by procrastinating doing important tasks that they find tedious.
From a biological perspective, we must understand the ADHD brain. People with ADHD have abnormal reward centers in the brain. They do not produce enough Dopamine. That is why stimulants help. Stimulants increase the release of Dopamine and also interfere with its breakdown. Therefore there is more Dopamine in the reward center. People with ADHD need higher levels of stimulation to get rewarded. Therefore anything that is highly stimulating helps them feel better. So the riskier the behavior the greater the stimulation and thereby the greater the Dopamine release, thus the greater the reward.
The problem I see is that therapists who treat addictions do not think about their patients having ADHD. The diagnosis is missed and treatment fails. Dr. Carnes and I noted that patients who fail addiction treatments often have untreated ADHD. This is also complicated because addiction programs do not like using medications at all. So my experience shows that adult therapists and Psychiatrists need to think about this disorder and be willing to treat it with medication. In my experience, patients with Sexual Addiction have more severe ADHD and require some type of medication to change their behavior. I have used Strattera( atomoxetine) and Intuniv(guanfacine) for this problem without the risk of stimulant abuse. I clearly do not believe that medicine should be the only treatment for this disorder. But my experience has shown me that is an important component along with a 12 Step Program as well as treating any other Psychiatric Axis I Disorders.
Your first therapy appointment is coming up and you’re nervous, “Is my therapist going to be weird? What’s she going to ask me? Am I going to find out I’m crazy?” First appointments are nerve-wrecking but they can be less so. Arm yourself with information and eliminate the majority of “the unknowns.” Here are some of the most important points to remember before meeting your new therapist.
1. Most people, even those that have had previous experience in therapy, feel nervous about coming to the first appointment with a new therapist. Whether it was your idea to come or not, it takes a lot of courage to talk to a therapist. How scary it is to sit face-to-face with a person you’ve never met before, telling him or her vulnerable details about your life! Part of the initial sessions in therapy involves exploring the question of “What does it feel like to be here, coming to therapy and seeking help?” It may feel like an ego hit to admit that you or your family is struggling and needs support. Each of us has a story to tell and that story becomes our reality; in times of struggle, we first have to recognize that something in our version of reality is not working. We grieve the reality that we have always known in order to be open to change which allows for the creation of a new reality. You may also be worried about being judged or if the information you reveal is really going to remain private and confidential. If you are 18 and older, what you say will remain confidential with the exception of the following situations: you are at risk of hurting yourself or others; someone you know is currently being hurt or is at risk for it; in some legal proceedings. If you are younger than 18, your guardians (usually your parents), have access to your records; however, good therapy is built on trust between you and your therapist, so the extent of what your therapist tells your guardians should be discussed and agreed upon as soon as possible. Parents, you can imagine that your child would be hesitant or unwilling to talk to his therapist if he knew that you would receive a play-by-play of the therapy session; thus, many therapists working with minors in individual therapy encourage the rule of not revealing the content of therapy unless the minor is at risk of hurting himself or others. For more information on privacy and confidentiality, visit http://www.apa.org/ethics/code/.
2. Being in therapy has been historically stigmatizing, but this is rapidly changing. In the past, psychology was about identifying and fixing a problem; in recent years, positive psychology has influenced therapists to consider what is working in a person’s life and find ways to maximize this success. Many therapists practice psychology by identifying a person’s strengths and work with the patient to help him/her use those strengths to overcome areas of struggle. Life is full of opportunities for beautiful experiences, but it is not always easy. We all face struggles at different points in our lives… it’s part of the human experience. Therapists can help you navigate the hardships and manage the stress. The better you are at managing your distress, the more available you are to enjoy.
3. Whether you have been to a therapist in the past or this is your first time, you are entering therapy with specific expectations and it is important to identify them. Most people who have had a previously disappointing experience with therapy did so because they expected therapy to be one way but experienced something else. Therapists’ approach to treatment is guided by their theoretical orientation. Most therapists are trained in a variety of theories that help them conceptualize what happens in therapy; most importantly, a therapist’s theoretical orientation influences how they behave in therapy and how they envision the patient should behave. A therapist who works from a cognitive behavioral therapy (CBT) approach is very directive in therapy, speaking a lot, educating, and giving homework assignments. On the other hand, a therapist specializing in psychoanalysis may listen more, resulting in the patient doing the majority of the talking, and will periodically make interpretations about what the patient is saying. A therapist who uses art therapy or psychodrama will encourage a patient to draw, create, speak to an empty chair, or act out hypothetical scenarios to work through a problematic situation. Imagine if you, as the patient, expected to do the majority of the talking with the therapist only occasionally chiming in with insightful interpretations… you may be turned off from therapy if your therapist begins assigning you homework or asking you to represent your emotions as a roller coaster in a drawing. The opposite is also true; if you expect your therapist to be very directive and hands on but you begin therapy with a therapist who mostly listens to you and occasionally makes interpretations, you may be disappointed because your expectations are not being met. Before your first appointment, think about your expectations and what you are looking for from your therapist; then, discuss your expectations with your therapist. Fortunately, most therapists are trained in many theoretical approaches and identify themselves as “eclectic,” pulling from many different theories as therapy progresses. My belief is that there is no “one size fits all” approach to therapy. Everyone is different and it is important for therapist to be flexible when working with distinct problems and diagnoses. Being able to pull from a variety of theories, each with their own interventions, allows a therapist to customize the therapy experience and honor the uniqueness of each patient. It is also important to identify your goals for therapy, keeping in mind that different participants may have different goals (i.e., young adults could have different goals from than their parents). A therapist can use an eclectic approach to address a variety of goals.
4. Cultural considerations are part of good therapy and they are important for everyone, not just people from other countries. Culture is commonly understood to mean the beliefs, attitudes, and behaviors of a group. We frequently hear the phrase “from a different culture” and our minds typically imagine something or someone from a different country. Though this mental leap is not wrong, we must consider that “different cultures” exist in our home country. The culture in the northeast of the United States is different from that of the south. Within the south, the culture in Texas is different from that of Mississippi. The culture in Houston is different from that of Temple. In addition to geographic location, culture is influenced by socioeconomic status, religion, ethnicity, race, sexual orientation, language, disability status, marital status, age group, and education level. Corporations have a company culture, schools have their own culture, and families have their own unique culture. A therapist is trained to consider these cultural factors in therapy and how they interact with and affect the patient. “Making assumptions” and being guided by cultural stereotypes is the first mistake to good multicultural treatment. As a psychologist with a passion for multiculturalism, my training and experience has taught me that we can never know everything about a specific culture; there are too many variables. Thus, for a therapist, the best approach to multicultural therapeutic work is to embody the spirit of curiosity, ask questions, and try to understand the uniqueness of each patient. As a patient, be open to exploring culture with your therapist so he/she can get to know your individual and special story as it is told by your specific combination of cultural factors.
5. If you are a parent bringing your child for treatment, it is important to remember that family involvement is crucial for sustained progress. Your child does not live in a bubble; rather, he/she lives in a family which influences and affects him. Each member of the family has his/her own individual life that may include going to school, work, church, spending time with friends which can all interact with one another. A husband’s day at work may affect his mood and stress levels which, in turn, affect his relationships within the family, familial duties, and also the child. A good therapist will explore these interrelated connections, so be open to exploring not just the factors directly related to your child, but also seemingly distant or seemingly unrelated factors that the therapist may ask you about. More information is always better than less, which relates to previous testing/evaluations; if your child had previously been evaluated by a speech therapist, an education specialist, or a psychologist, bring a copy of the results to help your new therapist understand the progression and history of the presenting problems.
Receiving a diagnosis can be scary, but a diagnosis is not necessarily set in stone. Psychological diagnoses and their criteria come from the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM 5). For insurance purposes, codes are given using the International Statistical Classification of Diseases and Related Health Problems, 10th revision (ICD 10). It is important to notice that the DSM is on its fifth edition and the ICD is on its 10th revision. Diagnoses and their criteria change as the fields of psychology and psychiatry discover new information through research and over time. When compared to the DSM-IV, the DSM 5 eliminated some of its diagnoses, changed criteria for others, collapsed some categories, and introduced new diagnoses. The original DSM was quite different from both the fourth and fifth editions. Providers qualified to give a diagnosis may be required to diagnose after the first appointment when information about a patient is incomplete, which speaks to the flaws in our medical system. Many of the diagnoses have overlapping symptoms and it can be difficult to pinpoint the exact diagnosis, especially after the first visit with limited information due to time constraints or other factors, like trust between patient and therapist.However, as therapists gather more information over time, they can alter the diagnoses. When working with children or developing young adults, diagnoses often change as developmental changes occur within the body. In addition, new research on brain plasticity tells us that our brains can change throughout life and can reorganize themselves to form new connections between brain cells. Diagnoses can be useful in identifying a problem and giving it a name so that appropriate treatment interventions can be applied; on the other hand, diagnoses are not very useful because they are susceptible to change. In short, rather than being overly concerned about a label (diagnosis), pay more attention to the problem areas and the symptoms. After all, diagnoses and their criteria in the DSM 5 and the ICD 10 can evolve, appear, and disappear, but the lived reality of your experience remains.
As you prepare for your first appointment, consider these six points and discuss them with your therapist. Remember, therapy is an interactive process and it is important for you to be an informed and active participant on your journey to well-being and managing your life.